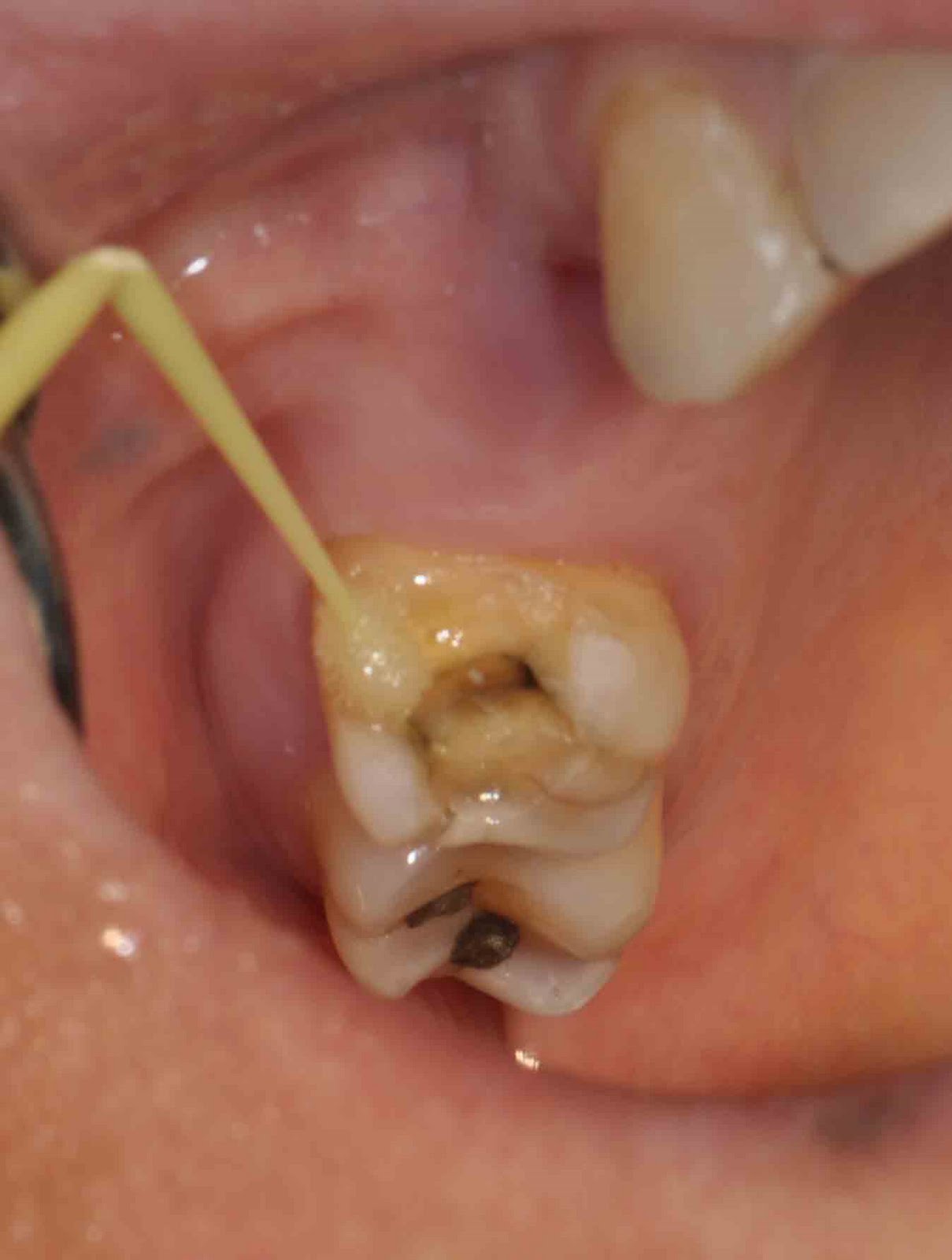
This young girl had an accident at home, causing two-third of her crown fractured and worse of all, the pulp of the tooth exposed.
We did an emergency root treatment over the tooth to reduce her pain and later on, build back the tooth (below)…
So, now she can smile confidently and pain free.
Oral health is integral to general health – from the Surgeon General’s Report on Oral Health, 2000
What is the association?
The mouth is directly connected to the body by the bloodstream and the digestive system
Left untreated, plaque and inflammation can lead to gingivitis
Untreated gingivitis may progress to periodontitis
Recent evidence suggests that periodontitis is associated with systemic diseases such as heart disease (eg. heart attack, stroke) and diabeties.
Prevention is better than cure
Daily Oral Care: Cleaning In Between
1. Dental Floss
Step 1
Step One:
Take about 18 inches (50cm) of floss and loosely wrap most of it around each middle finger (wrapping more around one finger then the other) leaving 2 inches (5cm) of floss in between
Step 2
Step Two:
With your tumb and index fingers holding the floss taut, gently slide it down between your teeth, while being careful not to snap it down on your gums.
Step 3
Step Three:
Curve the floss around each tooth in a “C” shape and gently move it up and down the sides of each tooth, including under the gumline
Air polishing is an alternative, non-contact, method of polishing teeth using a polishing cup and paste after teeth scaling. It requires a special ultrasonic unit (e.g. Air Flow from EMS) that allows use of this insert in the handpiece.
Air polishing uses medical-grade sodium bicarbonate and water in a jet of compressed air to “sandblast” the surface of the enamel smooth. Examples include the Prophy-Jet® and Cavitron Jet® (Dentsply Ltd.). The nozzle is held 3 to 5 mm from the tooth, centred on the middle third of the tooth. Use at 60° to the long axis of the root. Do not direct into the gingival sulcus.
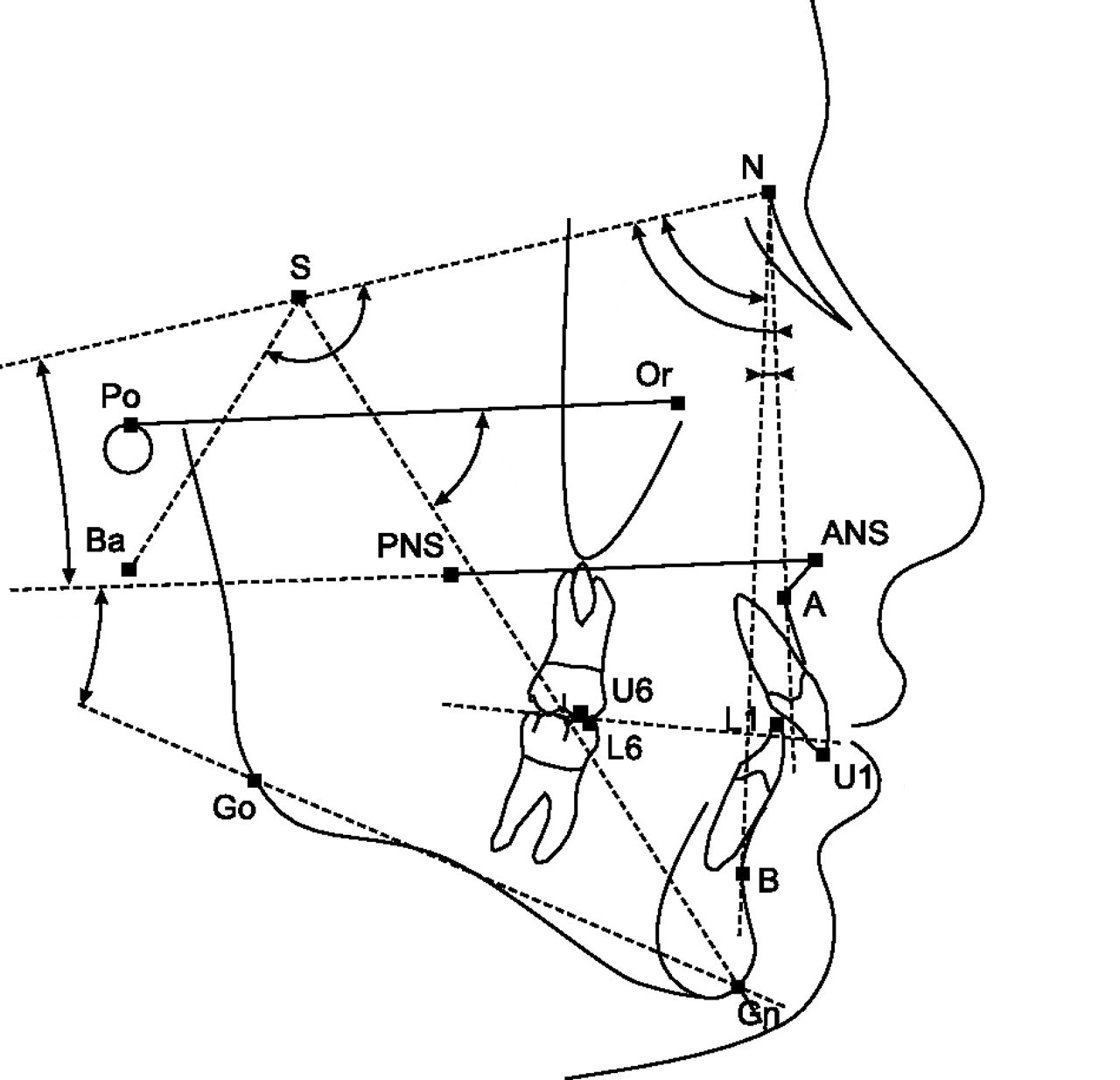
Lateral cephalometric is a radiograph of the head taken with the x-ray beam perpendicular to the patient’s sagittal plane. This radiography image is useful for studying the dental and facial growth of a patient.
Position of patient from the X-ray source to produce a standard Lateral cephalometric radiograph
In orthodontic treatment, clinician/orthodontist use this radiograph to identified dental and skeletal deformity; the relationship between upper and lower teeth and jaw bone. By doing so, he can create a treatment plan to correct the teeth misalignment. This radiograph is also useful in monitoring the progress of braces treatment and to compare before and after treatment.
Patient’ head is in ‘natural head position’
During radiograph taking, the patient’s head is positioned in the most relax position — natural head position — is a standardized orientation of the head that is reproducible for each individual and is used as a means of standardization during analysis of dentofacial morphology both for photos and radiographs.
An example of a standard Lateral Cephalometric Radiograph
Cephalometric Tracing
Cephalometric tracing is an overlay drawing produced from a cephalometric radiograph by digital means and a computer program or by copying specific outlines from it with a lead pencil onto acetate paper, using an illuminated view-box. Tracings are used to facilitate cephalometric analysis, as well as in superimpositions, to evaluate treatment and growth changes.
The landmarks on the radiograph are identified and marked.
Lines are made to join the markings and the angles where the lines intercept will be recorded. The values of the angle will be compared to the norm value according to the patient’s race. And finally, a conclusion will be depends on the deviation of the patient’s value to the norm value.
Sometimes, lateral cephalometric radiograph can be use to compare before and after treatment or the growth pattern of a child. For example, in the image below, the green line represent before treatment and the black will be after treatment. From here, we can appreciate how the teeth and jaws move during treatment. Doctor use this radiograph to evaluate if he has achieve his treatment objective!!
Primary teeth or Deciduous teeth, otherwise known as reborner teeth, baby teeth, temporary teeth and primary teeth, are the first set of teeth in the growth development of humans and many other mammals. In some Asian countries they are referred to as fall teeth as they will eventually fall out, while in almost all European languages they are called milk teeth as they exist when the child is still mainly drinking milk. They develop during the embryonic stage of development and erupt—that is, they become visible in the mouth—during infancy. They are usually lost and replaced by permanent teeth, but in the absence of permanent replacements, they can remain functional for many years.
Deciduous teeth start to form during the embryo phase of pregnancy. The development of deciduous teeth starts at the sixth week of development as the dental lamina. This process starts at the midline and then spreads back into the posterior region. By the time the embryo is eight weeks old, there are ten areas on the upper and lower arches that will eventually become the deciduous dentition. These teeth will continue to form until they erupt in the mouth. In the deciduous dentition there are a total of twenty teeth: five per quadrant and ten per arch. The eruption of these teeth begins at the age of six months and continues until twenty-five to thirty-three months of age. Usually, the first teeth seen in the mouth are the mandibular centrals and the last are the maxillary second molars.
The deciduous dentition is made up of central incisors, lateral incisors, canines, first molars, and secondary molars; there is one in each quadrant, making a total of four of each tooth. All of these are gradually replaced with a permanent counterpart except for the first and second molars; they are replaced by premolars. The replacement of deciduous teeth begins around age six. At that time, the permanent teeth start to appear in the mouth, resulting in mixed dentition. The erupting permanent teeth causes root resorption, where the permanent teeth push down on the roots of the deciduous teeth causing the roots to be dissolved and become absorbed by the forming permanent teeth. The process of shedding deciduous teeth and the replacement by permanent teeth is called exfoliation. This may last from age six to age twelve. By age twelve there usually are only permanent teeth remaining.
Teething age of deciduous teeth:
Central incisors : 6–12 months
Lateral incisors : 9–16 months
Canine teeth : 16–23 months
First molars : 13–19 months
Second molars : 22–33 months
Primary teeth care
Proper care of deciduous teeth is very important and starts at early stages even prior to their eruption. At the earliest stage, a child’s mouth and gums are to be wiped with a clean damp cloth, gauze pad, or especially designed teeth wipes. Wiping the baby’s teeth and gums after each feeding, and particularly at bedtime, helps prevent baby bottle tooth decay. This practice also helps reduce premature decay caused by harmful plaque-like film and bacteria that builds when babies ingest juices or any food containing sugar. Moreover, to reduce the possibilities to develop baby bottle tooth decay is it better to give the baby only plain water at bedtime or during the night and avoid juices, sugar water, milk or any other liquid containing sugar.
Non-flouride toothpaste
Once the first primary teeth come in, brushing starts. Warm water is normally used in these cases or a non fluoride toothpaste. The market offers special toothbrushes or finger toothbrushes for babies that help protect tender gums and gently clean baby teeth and gums. Other toothbrushes are specially designed for toddlers to easily grip them. They also come in catchy designs that encourage toddlers to use them. Toothbrush designs vary according to age, therefore, it is better to check the age recommendation on the package to obtain the most convenient one. Toothbrushes should be replaced every two to three months. It is also important to brush children’s teeth after giving them medicine as their acids may affect the tooth enamel. Early brushing helps reduce harmful bacteria, remove plaque, sugar, or any other kind of food that may cause tooth decay.
Reduce intake of high sugar food
Parents are advised to take their children to the first dentist visit when they are 12 months old. During this visit, the dentist can define dental care plan. Two possible ways to prevent tooth decay are the use of fluoride and sealants.
It is important to bring your children for dental check-up regularlyFluoride makes teeth stronger over time which then prevents the initiation of dental caries and tooth decay. Also, it re-mineralizes those areas of the teeth which have been weakened by acid. Fluoride can be included in one’s diet. Other ways of obtaining fluoride are in toothpastes and mouth rinses that are normally used at homes. The dentist can provide it through gels and foams he applies during dental visits.
To add to the benefits of the fluoride, dentists also apply sealant in order to preserve the teeth even more. Sealant is applied in some locations of the teeth that smooth their surface. Therefore, food and plaque are less likely to get trapped in those areas.
Children can start flossing when they are about 3-4 years old. However, at this age they might still need help and will be able to floss by themselves when they are 8-10 years old.
White filling or composite resin is getting more and more popular currently as it produces a nice aesthetic result. Previously silver filling (amalgam) is preferred due to low cost, easy to handle and it has a good mechanical properties (amalgam is strong and durable). However, current composite resin is as strong and durable as amalgam and on top of that, it produce a ‘hard to see restoration’ on the tooth making it a preferred choice for dentist and patient. Anyway, Nobody wants their filling to be seen!!
Composition of composite resin
Composite resins are composed of:
Bis-GMA monomers or some Bis-GMA analog
a filler material such as silica and in most current applications,
a photoinitiator
Dimethacrylates are also commonly added to achieve certain physical properties such as flowability.
Further tailoring of physical properties is achieved by formulating unique concentrations of each constituent.Unlike Amalgam which essentially just fills a hole, composite cavity restorations when used with dentin and enamel bonding techniques restore the tooth back to near its original physical integrity.
Variety of colours of composite resinsEmpress Direct – Highly aesthetic composite material
Dental composite resin
In our clinic, we have multiple shade (or colour) to choose to mimic the original colour of the tooth in the mouth. For every restoration, we use different shade for each ‘layer’ during restoration.
Below are some of the cases done in our clinic.
Restoring Composite Resin
(Illustration in great depth)
An old amalgam was removed from a upper right molar and the tooth was ready for filling placement
Firstly, the enamel surface of the molar was treated with phosphoric acid 35%
Then, it was followed by the dentine which was located at the center of the tooth
Next, the cavity was cleaned and dried. A thin layer of adhensive solution was applied over the cavity
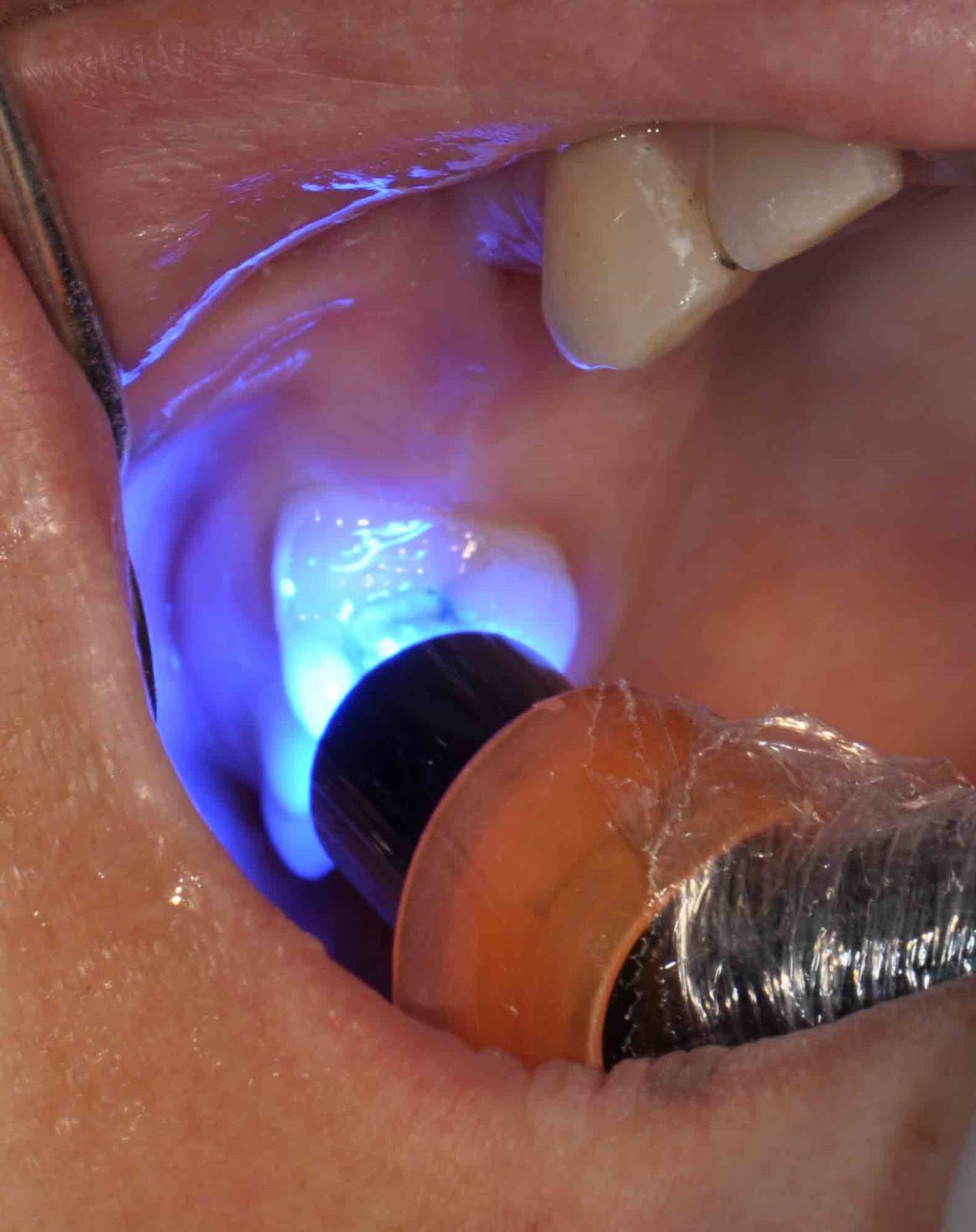
Light cure unit was used to activated the adhesive which was photo-sensitive
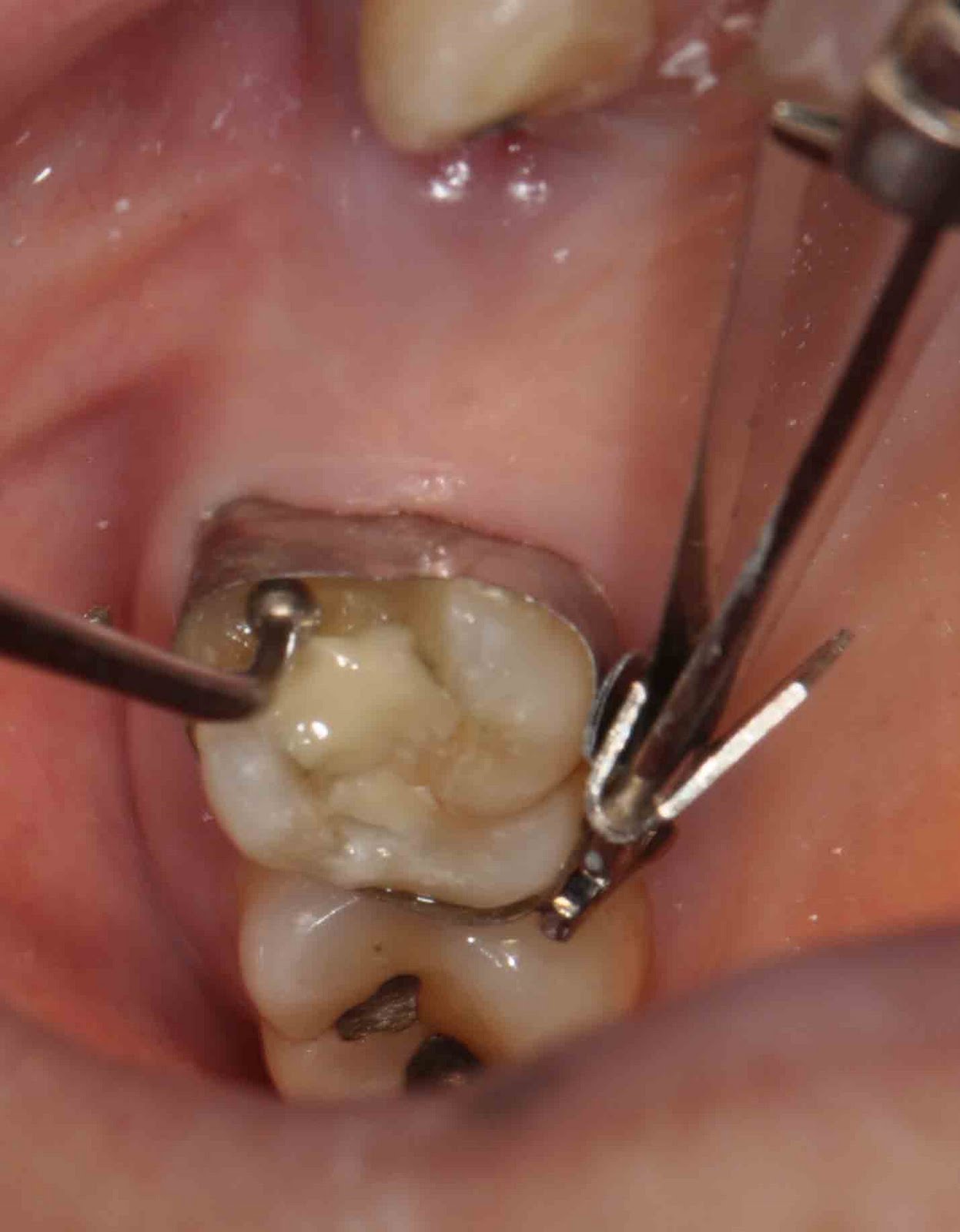
A metal band was used to wrapped around the molar
The metal band was checked to ensure that there was no gap between the tooth and the metal band. This was to prevent the filling material from overflow out from the cavity.
‘Dentine shade’ composite resin was placed at the center of the cavity to cover the darkish stain in the dentine area.
The composite was light-cured to make it harden
Next, ‘enamel shade’ composite was placed over the ‘dentine shade’ composite (layering technique) to get the translucency effect.
‘Enamel shade’ composite was placed at the side-wall of the molar and was cured (with light-cure unit)
The metal band was removed and more composite was placed at the side-wall of the molar so to achieve a nice contour and bulbosity.
This was the result after the composite harden
The composite excess was removed with a rotary white stone
The restoration was checked to look of any interference with the lower teeth during biting and chewing (with a bite registration tape)
And the red markings from bite registration tape was removed
Finally, for aesthetic reason, grooves and fissures was make on the tooth surface
And ‘stain’ composite was placed on the fissure to make it looked like the neighboor teeth
Lastly, light-cure unit used to harden the rest of the composite
The restoration was polished to make is glossy and shining
The Final Result!!
Before and after picture.
Another case: Replacing old silver (amalgam) restorations with composite restorations
This young gentleman came complaining of sensitive to hot and cold at his bottom right molars. On examination, he had a few siler fillings which cracked and had gaps noted at the margin fo the fillings.
The silver fillings were removed and replaced with white fillings. The fillings match with the colour of the tooth very well as if there was no filling done!!
Are Some People at More Risk for Developing Cavities?
How Can I Prevent Cavities?
What should I do if I have tooth decay?
What is Tooth Decay?
Dental cavities are an infection caused by a combination of carbohydrate-containing foods and bacteria that live in our mouths. The bacteria are contained in a film that continuously forms on and around our teeth. We call this film plaque. Although there are many different types of bacteria in our mouths, only a few are associated with cavities. Some of the most common include Streptococcus mutans, Lactobacillus casei and acidophilus, and Actinomyces naeslundii.
When these bacteria find carbohydrates, they eat them and produce acid. The exposure to acid causes the pH on the tooth surface to drop. Before eating, the pH in the mouth is about 6.2 to 7.0, slightly more acidic than water. As “sugary foods” and other carbohydrates are eaten, the pH drops. At a pH of 5.2 to 5.5 or below, the acid begins to dissolve the hard enamel that forms the outer coating of our teeth.
As the cavity progresses, it invades the softer dentin directly beneath the enamel, and encroaches on the nerve and blood supply of the tooth contained within the pulp.
Cavities attack the teeth in three ways:
1. Pit & Fissure
2. Smooth surface
3. Root surface
The first is through the pits and fissures, which are grooves that are visible on the top biting surfaces of the back teeth (molars and premolars). The pits and fissures are thin areas of enamel that contain recesses that can trap food and plaque to form a cavity. The cavity starts from a small point of attack, and spreads widely to invade the underlying dentin.
Decays formed at the the pits and fissures and spread to the whole biting surface of the teeth
The second route of acid attack is from a smooth surface, which is between, or on the front or back of teeth. In a smooth-surface cavity, the acid must travel through the entire thickness of the enamel. The area of attack is generally wide, and comes to a point or converges as it enters the deeper layers of the tooth.
At the smooth surface area, decay started in-between of the teeth
The third is the attack started at the root surface of the tooth after it was exposed to the oral cavity. The root is usually exposed due gum recession as a result of periodontitis (gum disease)
Decay at the root surface of the teeth
Recipe for tooth decay formation?
How Will I Know if I Have a Cavity?
The large majority of cavities are completely painless. This is because the outer enamel has no nerves. It is only when the cavity enters the underlying dentin that the cavity may begin to feel sensitive (Teeth sensitive). The most common cavity symptoms are an increased sensation to cold, sweet foods or beverages. A cavity is often responsible for a broken tooth. The cavity weakens the tooth, especially when it forms under a tooth filling or a tooth cusp, and can easily cause a fracture when biting down.
Sensitive Teeth
Patients are sometimes taken off guard when they learn that they have a few cavities but they don’t have any symptoms. It is far better to treat a small cavity than to wait until they have symptoms; such as pain. By the time there are symptoms, the cavity may have spread to infect the dental pulp, necessitating a root canalprocedure or a tooth extraction to eliminate the infection. Always remember that most dental problems are insidious — that is, they sneak up on you. Regular dental exams, at least twice a year, will greatly reduce the likelihood that a dental cavity will go undetected and spread, causing toothache pain and infecting the dental pulp.
The decay has spread into dental pulp causing pain
How Do Dentists Detect Cavities?
Cavities are detected a number of ways. The most common are clinical (hands-on) and radiographic (X-ray) examinations. During a clinical exam, the dentist uses a handheld instrument called an explorer to probe the tooth surface for cavities. If the explorer “catches,” it means the instrument has found a weak, acid damaged part of the tooth — a dental cavity. Dentists can also use a visual examination to detect cavities. Teeth that are discolored (usually brown or black), can sometimes indicate a dental cavity.
Regular dental examination is important to prevent tooth decay
Bite-wing radiograph is good to detect interproximal (in-between) caries
Dental X-rays, especially check-up or bitewing X-rays, are very useful in finding cavities that are wedged between teeth, or under the gum line. These “hidden” cavities are difficult or impossible to detect visually or with the explorer. In some cases, none of these methods are adequate, and a dentist must use a special disclosing solution to diagnose a suspicious area on a tooth.
Are Some People at More Risk for Developing Cavities?
People who have reduced saliva flow due to diseases such a Sjogren Syndrome; dysfunction of their salivary glands; have undergone chemotherapy or radiation; and who smoke are more likely to develop cavities. Saliva is important in fighting cavities because it can rinse away plaque and food debris, and help neutralize acid. People who have limited manual dexterity and have difficulty removing plaque from their teeth may also have a higher risk of forming cavities. Some people have naturally lower oral pH, which makes them more likely to have cavities.
How Can I Prevent Cavities?
The easiest way to prevent cavities is by brushing your teeth and removing plaque at least three times a day, especially after eating and before bed. Flossing at least once a day is important to remove plaque between your teeth. You should brush with a soft-bristled toothbrush, and angle the bristles about 45 degrees toward the gum line. Brush for about the length of one song on the radio (three minutes). It’s a good idea to ask your dentist or hygienist to help you with proper brushing methods.
Blushing and Flossing teeth are to do it daily to stop caries
Reducing the amount and frequency of eating sugary foods can reduce the risk of forming cavities. If you are going to drink a can of sweetened soda, for instance, it is better to drink it in one sitting, than sip it throughout the day. Better yet, drink it through a straw in one sitting, to bypass the teeth altogether. Getting to the dentist at least twice a year is critical for examinations and professional dental cleanings.
Reduce high sugar food can reduce dental cavity significantly
To reduce the incidence of cavities, use toothpaste and mouthwash that contains fluoride. Fluoride is a compound that is added to most tap water supplies, toothpastes, and mouth rinses to reduce cavities. Fluoride becomes incorporated into our teeth as they develop and makes them more resistant to decay. After our teeth are formed, fluoride can reverse the progress of early cavities, and sometimes prevent the need for corrective dental treatments.
Mouthwash with fluoride
The recent drop in the number of cavities is largely due to the addition of fluoride to our drinking water. Mass water fluoridation is the most cost-effective measure available to reduce the incidence of tooth decay. The Environmental Protection Agency has determined that the acceptable tap water concentration for fluoride is 0.7 to 1.2 parts per million.
A dental procedure called sealants can also help reduce cavities on the top and sides of back teeth (occlusal, buccal and lingual surfaces). A sealant is a white resin material that blankets the tooth, protecting the vulnerable pits and fissures of the tooth. Sealants are routinely placed on children’s teeth to prevent cavities on their newly developing molars. The use of sealants to prevent cavities is also a cost-effective way to reduce the incidence of cavities on adults as well. Sealants are generally not used on teeth that already have fillings.
Fissure Sealant
People who have a dry mouth are at risk for developing cavities, and can have their dentist prescribe artificial saliva and mouth moisturizers, as well as recommend chewing sugarless gum to stimulate saliva production. Finally, an antiseptic mouthwash containing chlorhexidine gluconate such as Chlohexxa or Oradex can also be useful in killing bacteria associated with dental caries.
What should I do if I have tooth decay?
You should go the to dental clinic as soon as possible. Early or small decay is easily to treat. Usually a small filling will do. However if it is large cavity, then a larger filling is required provided there is no pain. In cases where the tooth is painful (eg. pain on biting, disturb sleep), then root canal treatment or extraction is required to stop the infection. Small filling
Filling can be silver (amalgam) or white (composite). Large Filling
Usually required
Comparison within big and small filling:
Small Filling vs. Large filling
Less pain during filling More pain (because lager & deeper cavity)
More aesthetic Less aesthetic
More lasting and durable Less durable
Cheaper More expensive (more filling material)
Crown
Or tooth capping of is a procedure to created back function, aesthetic as well as protection to a severely damaged tooth. It is usually made of porcelain fused with metal or a full porcelain material. Crown is durable and more lasting compared to a large filling.
Crown
Root canal treatment (RCT)
RCT is required when infection from caries has spread to the pulp of a tooth. The tooth is usually painful on chewing and sometimes disturb sleep. The purpose of this treatment is to preserve the tooth by removing the dead and infected pulp leaving the tooth bacteria free.
After RCT, the tooth can be restored with filling or a corwn. If there is a lot of tooth structure loss, the tooth should be protected with a crown.
Root Canal Treatment
Extraction
Tooth extraction in another way to stop infection. However, this method is commenced if patient don’t want to keep the tooth anymore. Patient have to understand the consequent of removing the tooth
Root canal treatment vs. Tooth extraction
Dental filling is a dental restorative material used to restore the function, integrity and morphology of missing tooth structure. Basically… material used to fill up cavity in the tooth after the decay was removed from the tooth.
Most cavities discovered during a dental examination will need to be treated. In general, if a cavity has broken through the enamel and is into the underlying dentin, or is able to be probed with an explorer, it has undergone cavitation and requires treatment. Early dental cavities that have not spread to the dentin or have undergone cavitation should not be treated, as they can be healed or re-mineralized with fluoride.
The goal of treating cavities involves two basic principals:
1. Removing the decayed portion of the tooth
Teeth Decay
After the decay portion is removed and the tooth is ready for filling
2. Rebuilding the missing tooth structure with a filling material.
Filling material is used to replace missing tooth structure due to decay
The dentist usually begins the procedure with an injection of local anesthetic if the decay is deep and very sensitive. A high-speed dental drill is needed to remove the decay and prepare the tooth for the filling. Depending on which material is used, the dentist will vary the tooth preparation accordingly.
Dental drill (High-speed handpiece)
Decay is removed with a high-speed dental drill
After the tooth has been prepared, a liner (Dycal®)is often used to reduce tooth sensitivity.Dycal is a compound containing calcium hydroxide, and is used in deep cavities to stimulate the dentin to regenerate and protect the dental pulp. In deeper fillings, a base is used in addition to the liner. Common bases used under dental fillings are glass ionomer cement and zinc phosphate cement. The main purpose of the base is to insulate the tooth from temperature changes in the mouth. The dentist and patient can then choose a number of different materials to fill the tooth, but the most common are silver (amalgam), white (resin), porcelain or gold. These materials are layered on top of the liner or base to finish the process of rebuilding the tooth. After a tooth has been filled, it is not unusual for the tooth to be sensitive for a day or two. In general, the deeper the filling, the more likely the tooth will have prolonged sensitivity, especially to cold food or beverages. Most fillings should be completely comfortable within two weeks. In some cases, the filling will be built up too high, and a second appointment is needed to shave down the filling to a comfortable level. If sensitivity lasts more than two weeks, it may indicate that there is a void under the filling. Prolonged discomfort may also indicate a tooth that has an infected pulp, and requires root canal therapy.
What Dental Material is Best for My Teeth?
Dental Amalgam
Silver (Amalgam) Filling
Every dental material used to rebuild teeth has advantages and disadvantages. Dental amalgam or silver fillings have been around for over 150 years. Amalgam is composed of silver, tin, copper, mercury and zinc. Amalgam fillings are relatively inexpensive, durable and time-tested. On the flip side, they are considered unaesthetic because they blacken over time and can give teeth a gray appearance, and they do not strengthen the tooth. Some people worry about the potential for mercury in dental amalgam to leak out and cause a wide variety of ailments, but research does not bear this fear out. Advantages:
Cheap
Strong
Lasting
One visit
Disadvantages:
Not aesthetic (Silver colour)
Blacken over time and can give the teeth a gray appearance
Contain mercury
Required deeper cavity to retain amalgam
No chemical bonding to tooth structure
Composite Resin/White Filling
White (Composite Resin) Filling
Composite resin, or white fillings have been around for about two decades. Composite fillings are composed of an organic polymer known as bisphenol-A-glycidyl methacrylate (BIS-GMA), and inorganic particles such as quartz, borosilicate glass and lithium aluminum silicate. They have the advantage of requiring a more conservative tooth preparation (less drilling required), can have a strengthening effect on the tooth and are very aesthetic, virtually blending in with the tooth. Composite fillings are the material of choice for repairing the front teeth. On the down side, they are more technique-sensitive for the dentist to place, and are highly susceptible to decay in the future if placed improperly. They usually cost more than an amalgam. Despite this research composite fillings are considered safe, and like the other dental filling materials, they are approved by the American Dental Association. Advantages:
Highly aesthetic – it can be used to improve aesthetic
Can be used for shallow cavities
Chemically bond to tooth structure
One visit
Disadvantages:
Technique sensitive (required dry surface for filling adhesion)
Can result in tooth sensitivity (due to shrinkage of the composite)
The strength of composite is lesser than amalgam
Required replacement or repair due to staining, chipping, wear and tear
Porcelain onlay used to formed back missing tooth structurePorcelain crownPorcelain crown
Porcelain is sometimes used for dental fillings called onlays or inlays. Porcelain is a non-crystalline glass composed of silicon and oxygen. It has the advantage of being highly aesthetic, and is the restoration of choice for people who place the highest value in the appearance of their teeth. Porcelain has the disadvantage of being brittle, and, therefore, susceptible to breakage. It is also even more technique-sensitive to use than composite; requires two dental visits to place the filling; and costs significantly more than amalgam or composite fillings. Porcelain can also cause accelerated wear of the opposing tooth when biting. Advantages:
Highly aesthetic
Strong
Lasting
Disadvantages:
Required to scarified more tooth structure for retention
The retention of the porcelain is depends on the cement used to ‘glue’ the porcelain to the tooth
Porcelain is brittle and susceptible to breakage
Required two visits
Can cause accelerated wear of the opposing tooth when biting
Gold onlay
Gold is sometimes used for dental fillings, most commonly as an inlay. Gold is not used in its pure form, but as an alloy containing 75 percent gold, as well as copper, silver, platinum, palladium and zinc. Gold is extremely durable; fairly aesthetic, it does not damage the opposing tooth when biting, and is very well tolerated by the gums and other intraoral tissues. A well-done gold filling can last two to four times longer than any other dental material and might be considered the “gold standard” for dental fillings. Gold inlays, like porcelain inlays, take two dental visits to complete and are also much more costly than amalgam or composite. They are also not nearly as aesthetic as composite or porcelain. In addition, gold inlays are fairly difficult to prepare and place.
Advantages:
Durable
Strong
Lasting
Very well tolerated by the gums and other intraoral tissues (bio compatibility)
Does not damage the opposing tooth when biting (as compared to porcelain)
Disadvantages:
Not aesthetic
Difficult to prepare
Required to scarified more tooth structure for retention
Book an appointment with our doctors now!! Click here
If you have any question, don’t hesitate to contact us, we are more than glad to provide you with the information you need!
![Composite-Build-up-01 [1600x1200]](https://prestige-dental-care.com.my/wp-content/uploads/2013/04/Composite-Build-up-01-1600x1200.jpg)
![Composite-Build-up-11 [1600x1200]](https://prestige-dental-care.com.my/wp-content/uploads/2013/04/Composite-Build-up-11-1600x1200.jpg)
![Composite-Build-up-12 [1600x1200]](https://prestige-dental-care.com.my/wp-content/uploads/2013/04/Composite-Build-up-12-1600x1200.jpg)













![Consultation01 [1600x1200]](https://prestige-dental-care.com.my/wp-content/uploads/2011/02/Consultation01-1600x1200.jpg)

















")
")






























 caries")












")

 Filling")
 Filling")




 :
:  :
: 