Braces treatment (Orthodontic treatment) is used to correct the teeth alignment prior to jaw surgery (Orthognathic surgery) for patients with discrepancy in his jaw relationship. This procedure requires close collaboration between orthodontist (dentist who does braces treatment) and maxillofacial surgeon (dentist who does jaw surgery). The objective of braces treatment before jaw surgery is to prepare the patient for surgery by placing the teeth in correct position in relative to their respective jaw bone without concern for the bite and aesthetic of patient. During this phase, patient might have compromised aesthetic and bitting ability until the jaw surgery is done. After jaw surgery, short duration of braces treatment is required to refine the final occlusion.
Reasons of braces treatment before jaw surgery
Facilitate the surgical procedures
Allow maximum surgical correction
Shorten and simplify braces treatment after the surgery
Allow production of stable bite during and after surgery
Oral cysts and tumors may develop in the jawbone or soft tissues in the mouth and face. Oral cyst is an abnormal cavity within bone or soft tissues which may contain fluid. There are many different types of cysts in the mouth.
Reason to remove oral cyst:
Size of cyst will increase with time
Very large cyst can be dangerous, they can weaken your jawbone and causes your jawbone to be break easily
Teeth adjacent to large cyst can be affected and become mobile
Oral tumor is a solid or semi-solid mass in the bone or soft tissue that is made of unusual cells. Oral tumor can be benign tumor (not cancerous) or malignant tumor (cancerous). This can be confirmed by using biopsy test (a surgery that removes part of your tumor to examine it under a microscope). Biopsy is needed to diagnose the tumor before starting any treatment.
When should I suspect that I have an oral cyst or tumor? Most of the oral lesions do not have any symptoms. Oral cyst may cause swelling, bone expansion, displacement or loosening teeth and pain (if infected). Oral tumor may present as a non-painful bump, lump, or ulcer. After your oral and maxillofacial surgeon examines the cyst or tumor, he will often recommend an X-ray to determine what kind of treatment you need.
Type of common treatments for oral tumors and cysts – Treatment options depends on the location and the type of lesion and your symptoms.
Fine needle aspiration cytology (FNAC): FNAC is a fast and less invasive tool used to diagnose a suspicious lesion or to differentiate cancerous and non-cancerous lesion before any invasive surgery done. This technique uses fine needle to obtain cells from lesion for examination under a microscope or to explore whether a lesion contains a fluid.
Surgical excision: Complete removal of lesion with the surrounding normal tissues.
Incisional biopsy: This technique removes only a small portion of a large lesion for diagnosis prior to treatment. Incisional biopsy indicated in very large lesion, hazardous location of the lesion and lesion that has the characteristics of malignancy.
Enucleation: A technique used to completely remove cyst by elevating of soft tissue flap, removing of bone overlying the cyst followed by peeling off the cyst with spoon-like instrument.
Marsupialization: Removes only a portion of the cyst lining and the cystic lining is sutured to the oral mucosa to keep the cavity open. The open cavity will trap food and takes many months to heal. This technique rarely used, unless associated structures, such as adjacent nerve, nose, and maxillary sinus are at the risk of damage during enucleation.
Multiple dental extraction is defined as removal of more than one tooth in a single dental visit. This procedue usually will be done under general anaesthesia (GA) in the hospital setup. Dental extraction under GA also can be performed on children who is anxious, uncooperative or having medical condition such as cerebral palsy or hyperactive child. In some cases, dental extraction under GA is done on children with badly decay teeth which needed multiple dental visit for extraction. It is therefore, better to have it done under general anaesthesia.
The indications of dental extractions under general anesthesia are:
Young child with rampant decayed teeth
Children who is unsuitable for local anesthetic or conscious sedation due to lack of cooperation
Patient with medical condition such as cerebral palsy or severe seizure
Patient who required lot of tooth extraction
Dental extraction under GA di performed in the hospital setup as day-care (no hospitalization). The patient (or the child) is usually health (ASA I) and fasting since midnight. The anesthesiologist will assess the child and written consent is taken before the procedure started.
In the operating room, the anesthesiologist will put a tube in patient’s throat to administer ‘sleeping’ gas allowing patient to ‘sleep’ during the whole procedure. The oral surgeon will come in to perform the dental extraction. After the procedure, the tube with be removed from the patient’s throat, and he will placed in the recovery room. He will be allowed to discharge from the hospital when fully conscious and ambulated.
Upon the procedure, a minor bleeding in extraction site, swollen tongue/lip/chin/cheek, temporary mouth opening limitation are the sequelae or conditions to be expected.
Advantage of extraction under GA
Very useful to traet uncooperative patient
Patient has no experience of the awlful dental extraction
No need many dental visit for extraction
Other dental procedures such as fillings and dental cleaning can sometimes be done in the same visit
Disadvantage of extraction under GA
Patient has to be healthy for GA
The procedure has to be done in the hospital setup with OT facility
Treatment will cost more as the patient has to be admitted in the hospital as well as GA fees
In general anesthesia (GA), drugs are administered by intravenous or inhalation routes which makes the person to be unconscious and do not feel or remember anything during the surgery. This patient is not wakened even by painful stimulation. General anaesthesia currently can only be performed in the operating room under the hospital setup where the sleep doctor (anaesthesiologist) will be the one to make the patient sleep.
GA is recommended for:
Complicated, extensive, and prolonged treatment to be performed
Working in difficult or multiple areas in the mouth
Patient with special needs
Uncooperative patient
Patient with extremely dental anxiety – only if other form of sedation are ineffective
Advantages
The patient is unconscious – allows the dentist to perform surgery without concern of constantly moving, uncooperating or anxiety patient.
Patient do not feel pain
Patient cannot remember events occurred during the surgery
Longer operating time
Disadvantages
The patient is unconscious – can be life threatening
Higher risk of complications – higher risk of airway obstruction because patient unable to cough
Patient cannot control the situation – do not respond to sound and touch
Require assistant to maintain a patent airway – patient cannot breathe on his own
Very expensive – require special equipment
Patient must fast at least 8 hours before surgery
Requires adequately and specially trained doctor (anesthesiologist) to perform
Time consuming procedure – long recovery period
Procedures
Before administering GA, the patient should be assessed thoroughly by the anesthesiologist by taking detailed medical history, drug history, physical test, and extensive laboratory test. The patient should be explained about the procedure and informed consent form should be signed by the patient. Patient must fast at least 8 hours before the procedure.
Then, GA drug administered intravenously or by inhalation to induce general anaesthesia.
After GA is induced, the doctor will secure your airway by placing a tube into your lung via the nose, mouth or a opening in the neck to ensure sufficient oxygen to reach your lung before dental treatment begins.
When dentist has finished the dental treatment, the doctor will stop the administration of GA drugs and begins to bring the patient back to consciousness. The patient should be monitored for 1-2days before discharging.
The uses for general anesthesia in dentistry have decreased over the years as other less invasive sedation techniques have evolved. Nevertheless, there are still many situations that require the use of GA.
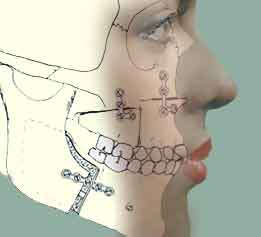
A young lady came to our clinic complaint that she was not happy about her face because of her lower jaw was too long. On top of that, her teeth weren’t aligned well. After examination and a few x-ray, we found that she had a few problems:
Her lower jaw was long as compared to her cranial base
Her upper jaw was shorter in relation to her cranial base
Her cheek looked more flatten
She can’t close her lips as her lower jaw as too forward
Her lower teeth were very far forward as compared to her upper teeth
Her dental mid-line was not coincide with her face mid-line
Corrective jaw, or orthognathic, is a surgery performed by the Oral and Maxillofacial Surgeons aimed to correct wide range of skeletal irregularities that cause disharmony in teeth and facial facial appearance; as well as interfering speaking and reduce chewing efficiency, and worst of all, obstruct breathing. Beside enhancing patient’s appearance dramatically, orthognathic surgery is also performed to correct functional problems.
Electrosurgery is the application of a high-frequency electric current to biological tissue as a means to cut, coagulate, desiccate, or fulgurate tissue. (These terms are used in specific ways for this methodology—see below). Its benefits include the ability to make precise cuts with limited blood loss. Electrosurgical devices are frequently used during surgical operations helping to prevent blood loss in hospital operating rooms or in outpatient procedures.
In electrosurgical procedures, the tissue is heated by an electric current. Although electrical devices may be used for the cauterization of tissue in some applications, electrosurgery is usually used to refer to a quite different method than electrocautery. The latter uses heat conduction from a probe heated to a glowing temperature by a direct current (much in the manner of a soldering iron). This may be accomplished by direct current from dry-cells in a penlight-type device. Electrosurgery, by contrast, uses alternating current to directly heat the tissue itself. When this results in destruction of small blood vessels and halting of bleeding, it is technically a process of electrocoagulation, although “electrocautery” is sometimes loosely and nontechnically used to describe it. (Source from Wiakipidia)
Electrosurgery unit
Using electrosurgery in oral surgery procedures
Electrocautery is a very useful tool to make a cut or excise soft tissue just like a scaple blade does. While a cut is made; at the same time, electrosurgery coagulate the surrounding blood vessels make surgery bloodless. This will improve visibility during surgery and less blood loss. More over, healing of a wound with electrosurgery is proven to be faster that wound made by scaple blade.
Electrosurgery: Coagulating the gum area before impression taking during tooth preparation for crown fabrication
Dental procedure which can be done with
Excision of lesions (eg. cysts, tumors)
Gum surgery
Implant placement
Crown lengthening
Coagulating the gum area before impression taking during tooth preparation for crowns/bridges
Advantages of using electrocautery
Less bleeding
Can be use to control bleeding
Wound heal faster with electrosurgery than using scaple blade
An oral and maxillofacial surgeon is a regional specialist surgeon treating the entire craniomaxillofacial complex: anatomical area of the mouth, jaws, face, skull, as well as associated structures.
In the US, the name oral and maxillofacial surgery should be abbreviated most appropriately as OMS, rather than OMFS as some sources suggest. The abbreviation OMFS may be appropriate only in the European system where Maxillo-Facial is hyphenated. In the US, maxillofacial is the official entry in the American language dictionary defining the anatomical region, and is also the official term used by all related surgical organizations, including the AAOMS, ABOMS, and ACOMS.
Maxillofacial surgeons are usually initially qualified in dentistry and have undergone further surgical training. Some OMS residencies integrate a medical education as well and an appropriate degree in medicine (MBBS or MD or equivalent) is earned, although in the United States there is legally no difference in what a dual degree OMS can do compared to someone who earned a four year certificate. Oral & maxillofacial surgery is universally recognized as a one of the nine specialties of dentistry. However also in the UK and many other countries OMFS is a medical specialty as well culminating in the FRCS (Fellowship of the Royal College of Surgeons). Regardless, all oral & maxillofacial surgeons must obtain a degree in dentistry (BDS, BDent, DDS, or DMD or equivalent) before being allowed to begin residency training in oral and maxillofacial surgery.
They also may choose to undergo further training in a 1 or 2 year subspecialty fellowship training in the following areas:
Head and neck cancer – microvascular reconstruction
Cosmetic facial surgery
Craniofacial surgery/Pediatric Maxillofacial surgery
Cranio-maxillofacial trauma
Head and neck reconstruction (plastic surgery of the head and neck region)
Maxillofacial regeneration(reformation of the facial region by advanced stem cell technique)
The popularity of oral and maxillofacial surgery as a career for persons whose first degree was medicine, not dentistry, seems to be increasing in few EU countries However the public fund spend for 14 years of training is a big concern of the state. Integrated programs are becoming more available to medical graduates allowing them to complete the dental degree requirement in about 3 years in order for them to advance to subsequently complete Oral and Maxillofacial surgical training.
Surgical procedures
Treatments may be performed on the craniomaxillofacial complex: mouth, jaws, neck, face, skull, and include:
Dentoalveolar surgery (surgery to remove impacted teeth, difficult tooth extractions, extractions on medically compromised patients, bone grafting or preprosthetic surgery to provide better anatomy for the placement of implants, dentures, or other dental prostheses)
Diagnosis and treatment of benign pathology (cysts, tumors etc.)
Diagnosis and treatment (ablative and reconstructive surgery, microsurgery) of malignant pathology (oral & head and neck cancer).
Diagnosis and treatment of cutaneous malignancy (skin cancer), lip reconstruction
Diagnosis and treatment of congenital craniofacial malformations such as cleft lip and palate and cranial vault malformations such as craniosynostosis, (craniofacial surgery)
Diagnosis and treatment of chronic facial pain disorders
Diagnosis and treatment of temporomandibular joint (TMJ) disorders
Diagnosis and treatment of dysgnathia (incorrect bite), and orthognathic (literally “straight bite”) reconstructive surgery, orthognathic surgery, maxillomandibular advancement, surgical correction of facial asymmetry.
Diagnosis and treatment of soft and hard tissue trauma of the oral and maxillofacial region (jaw fractures, cheek bone fractures, nasal fractures, LeFort fracture, skull fractures and eye socket fractures).
Splint and surgical treatment of sleep apnea, maxillomandibular advancement, genioplasty (in conjunction with sleep labs or physicians)
Surgery to insert osseointegrated (bone fused) dental implants and Maxillofacial implants for attaching craniofacial prostheses and bone anchored hearing aids.
Cosmetic surgery limited to the head and neck: (rhytidectomy/facelift, browlift, blepharoplasty/Asian blepharoplasty, otoplasty, rhinoplasty, septoplasty, cheek augmentation, chin augmentation, genioplasty, oculoplastics, neck liposuction, lip enhancement, injectable cosmetic treatments, botox, chemical peel etc.)
They are the last molar (or third molar) that usually erupt at the age of 18 to 25 years old (and sometimes older). The eruption of the tooth may cause pain in some of the cases. There are usually 4 wisdom teeth in each person. However, in some cases not every tooth will erupt into the oral cavity.
Impacted Wisdom Teeth
When a wisdom tooth cannot erupted properly either it tilt to the front or back or half-way jammed it is consider as impacted. The impaction cause severe pain especially when the tooth is erupting. This prevents the patient from open his mouth wide or eat properly. Sometimes it interferes with his daily activities. Impaction of wisdom tooth also will cause food trap easily (between the second last molar and wisdom teeth) which will result in decay at the second molar.
Impacted wisdom teeth can be divided into one of several categories. Mesioangular impaction is the most common form (44%), and means the tooth is angled forward, towards the front of the mouth. Vertical impaction (38%) occurs when the formed tooth does not erupt fully through the gum line. Distoangular impaction (6%) means the tooth is angled backward, towards the rear of the mouth. And finally, Horizontal impaction (3%) is the least common form, which occurs when the tooth is angled fully ninety degrees sideways, growing into the roots of the second molar.
Impacted wisdom teeth may also be categorized on whether they are still completely encased in the jawbone. If it is completely encased in the jawbone, it is a bony impaction. If the wisdom tooth has erupted out of the jawbone but not through the gumline, it is called a soft tissue impaction. Sometimes the wisdom tooth fails to erupt completely through the gum bed and the gum at the back of the wisdom tooth extends over the biting surface, forming a soft tissue flap or lid around the tooth called an operculum. Teeth covered by an operculum can be difficult to clean with a toothbrush.
Signs and Symptoms of Impacted Wisdom Tooth
Usually impacted wisdom teeth are presented with:
Pain
Gum Swelling
Cheek swelling
pain (may disturb sleep and may extend to the back, neck and head)
unable to open the mouth big due to pain
infection of the gum around the wisdom tooth
swelling on the gum
swelling on the cheek of the affected side
fever
Consequence of impacted wisdom teeth
Impacted wisdom tooth can lead to:
Acute gum infection or pericoronitis that happens around the wisdom tooth (Most common).
Infection on the pulp or pulpitis in the wisdom teeth due to decay
Infection on the pulp or pulpitis in the second molar due to prolong food trap that causes dental caries.
Infection on the bone or osteomylitis which occur if infection spread into the bone.
Infection around the facial tissue or cellulitis. This happens when the infection spread into the soft tissue around the facial region (Below).
Facial cellulitis
Gum abcess – if pus present in the gum or facial abcess if it’s in the face region
Gum problem or periodontitis around wisdom tooth and second molar.
Treatment Options
1. Leave it – If the symptoms are very mild, usually with some mouth rinse and the pain will subside. However, sometimes the pain may come back due to re-infection. 2. Take antibiotic and pain killer – Again the symptoms will subside however re-infection still can occur.
Antibiotics
3. Incisional and Drainage – Removing of the pus accumulated either in the gum or facial region then followed by removing of the wisdom tooth. 4. Operculectomy – Removing the gum that cover the wisdom tooth for easy cleaning. However, sometimes the gum might grow back and infection can re-occur
Operculectomy procedure
5. Extraction – Removing the wisdom tooth (surgery or without surgery)
Extraction
6. Root canal treatment – On the second molar if the pulp is infected and the wisdom tooth required to be removed.
Indication of Wisdom teeth Extraction
Wisdom teeth are extracted for two general reasons: either the wisdom teeth have already become impacted, or the wisdom teeth could potentially become problematic if not extracted. Potential problems caused by the presence of properly grown-in wisdom teeth include infections caused by food particles easily trapped in the jaw area behind the wisdom teeth where regular brushing and flossing is difficult and ineffective. Such infections may be frequent, and cause considerable pain and medical danger.
According to NICE (The National Institute for Clinical Excellence – UK), the routine practice of prophylactic removal of pathology-free impacted third molar should be discontinued. Third molar should be removed if there is evidence of pathology includes unrestorable caries, non-treatable pulpal and/or periapical pathology, cellulitis, abcess and osteomyelitis, internal/external resorption of the tooth or adjacent teeth, fracture of tooth, disease of follicle including cyst/tumour, tooth/teeth impeding surgery or reconstructive jaw surgery, and when a tooth is involved in or within the field of tumour resection.
Pericoronitis
The degree to which the severity or recurrence rate of pericoronitis should influence the decision for surgical removal of a third molar remains unclear. The evidence suggests that a first episode of pericoronitis, unless particularly severe, should not be considered an indication for surgery. Second or subsequent episodes should be considered the appropriate indication for surgery.
Surgery or Not Surgery?
When a wisdom tooth erupts vertically just like the second molar and the access is easily, then extraction of the tooth will be straight forward case. Usually the surgeon will loosen the tooth and grip the tooth with a forceps to remove it.
Horizontal impaction of wisdom tooth
However, most of the impacted wisdom tooth is embedded in the bone, tilted either forward or backward. Sometimes the tooth is in a horizontal position instead of vertical. This will make extraction with forceps impossible. Therefore, surgery is required.
Surgical Removal of Wisdom Tooth
Usually done by a oral surgeon (Specialist) or an experience dentist and it should be done in a sterile manner. After injections are given, a small cut will be made on the gum to expose the wisdom tooth and bone surrounding it. Then some bone near to the tooth will be removed to allow instrument to engage with the tooth. Next, the tooth will be sectioned into half or more and the fragment of tooth will be removed.
After the whole tooth was removed completely, the socket will be cleaned and the surgeon will inspect the wound to make it is clean and bleeding stop. Finally, the gum will be held together by stitches and the patient will be allowed to go home with gauze, pain killer and antibiotic. Usually the whole process takes about an hour or less.
For Anxiety Patient…
If in a case of an anxious patient come for wisdom tooth surgery, usually, we will prescribe some medication of reduce anxiety before the surgery or patient will have to inhale nitrous oxide during the procedure so that he/she will feel relax and calm all the time during surgery. If the patient is extremely phobia of surgery, then he can opt for surgery done under general anaesthesia which required hospitalization.
What Do I Need to Do During Recovery?
After your wisdom teeth are removed you may experience some swelling and mild discomfort, which are normal symptoms and are part of the healing process. Here is what to expect after the procedure. 1) The First 24 Hours:
Bleeding: This may occur for several hours after your wisdom teeth are removed. To control it, place a piece of clean moist gauze or moistened tea bag over the empty tooth socket and bite down firmly. This needs to be done for about 45 minutes. You should avoid rinsing, spitting or sucking actions for 24 hours after your wisdom teeth are removed. For example, don’t drink beverages through straws or smoke, and avoid hot liquids (such as soup or tea). You should also avoid carbonated and alcoholic drinks. These activities can cause the clot to dislodge, which will cause dry socket.
Facial Swelling: This can occur where the wisdom tooth was extracted. You can apply a cold compress to ease the swelling and pain. Cold compress(ice packs) should be used 20 minutes on 20 minutes off. Repeat as necessary during this first 24-hour period. Avoid taking aspirin, ibuprofen (e.g. Motrin, Advil, etc.) if you have a stomach ulcer.
Pain: Medications such as Mefenamic Acid (Ponstan) or Etoricoxib (Arcoxia) can be taken to manage your pain. We may prescribe more potent pain relievers, such as narcotics, if necessary.
Antibiotics: Antibiotics may be prescribed post-treatment and should be taken until you have finished the prescription.
Food: Avoid hot liquids and alcoholic beverages for at least 24 hours. When the extraction is more difficult, you will need to consume a soft or liquid diet for at least 24 hours after removal of your wisdom teeth.
Brush your Teeth: You need to continue to brush your teeth, but avoid the teeth adjacent to the extracted tooth during the first 24 hours. On day two, you can resume the gentle brushing of your teeth. However, do not use commercial mouth rinses because these can irritate the area of extraction. 2) After 24 Hours:
Facial Swelling: Facial Swelling in the area of your wisdom tooth extraction needs to be man aged with heat after the first 24 hours of ice. Use a moist warm towel and apply it to the area on a 20-minute on, 20-minute off schedule. Repeat as necessary.
Rinse Your Mouth with Warm Salt Water: Use 1/2 teaspoon of salt in a cup of warm water after before bed and after meals. Do not use commercial mouth rinses.
Complete Healing: This will not occur for a few weeks to a few months following the removal of your wisdom teeth. However, usually within the first week or two, you will feel reasonably comfortable because enough healing has taken place. We will explain what to expect regarding your healing process.
Complication of Wisdom Tooth Surgery
1) The usual problem the patient will experience after surgery
Pain on surgical site
Limited mouth opening
Swelling around the cheek
Bruise over the cheek (not usual)
2) Complication (Rare!!)
Infection on surgical site (Higher risk for smoker and diabetic patient)
Lower jaw fracture (Will only happens in very thin jaw or a rough surgery)
Bleeding (Can be from arteries which usually can be controlled with compression)
Injury to nerve (Damage to the nerve will happens when the wisdom tooth is very near to the nerve and the event of removing it cause injury to the nerve. This will result in numbness on the lower lipand usually it takes 6-12 months to recover.)
Dental implant is an artificial root of the tooth used in dentistry to support restorations that resemble a tooth or group of teeth.
All dental implants today (21st century) are root-form and they are placed inside the bone (endosseous implant). Prior to the advent of root-form endosseous implants, most implants were either blade endosseous implants, in that the shape of the metal piece placed within the bone resembled a flat blade, or subperiosteal implants, in which a framework was constructed
Implant is used to support a crown (for the case of missing a single tooth) or they can be used to support bridge or denture (for the case of multiple missing teeth) that are designed to look just like your natural teeth.
Dental implants are small screws made of pure titanium that are surgically implanted in your jaw.
They provide a permanent foundation for crowns, bridges and dentures.
They are proven technology backed up by more than 50 years of development.
Dental implants protect your jaw against bone loss.
Because dental implants anchor in the jawbone just like natural teeth, they are the best choice for natural-looking tooth replacement
Composition of an Implant
A typical implant consists of a titanium screw (resembling a tooth root) with a roughened or smooth surface. The majority of dental implants are made out of commercially pure titanium, which is available in 4 grades depending upon the amount of carbon and iron contained. More recently grade 5 titanium has increased in use which offers better tensile strength and fracture resistance. Implant surfaces may be modified by plasma spraying, anodizing, etching or sandblasting to increase the surface area and the integration potential of the implant.
Anatomy of Implant
Implant/Fixture – titanium material for osteo-integration with the surrounding bone. Abutment – structure which connects the implant to the crown and it is situated in the gum area. Crown – Usually porcelain fused to metal material that can be seen in the mouth. What is the difference between dental implant and natural tooth?
Who should perform the Implant placement?
Implant surgery may be performed as an outpatient under general anesthesia, oral conscious sedation, nitrous oxide sedation, intravenous sedation or under local anesthesia by trained and certified clinicians including general dentists, oral & maxillofacial surgeons, prosthodontists, and periodontists.
Surgical procedure
Surgical planning
Prior to commencement of surgery, careful and detailed planning is required. Two-dimensional radiographs, such as orthopantomographs (OPG) or periapicals radiograph are often taken prior to the surgery. They are used to identify vital structures (such as the inferior alveolar nerve or the sinus), as well as the shape and dimensions of the bone to properly orient the implants for the most predictable outcome. In some instances, a Cone beam tomogram (CBT) or CT scan will also be obtained.
Jaw X-ray — Dental Panaromic Tomogram (or OPG)
Cone Beam Images of the jaw bone
Implant placement procedure
In its most basic form the placement of an osseointegrated implant requires a preparation into the bone using either hand osteotomes or precision drills with highly regulated speed to prevent burning or pressure necrosis of the bone. After a variable amount of time to allow the bone to grow on to the surface of the implant (osseointegration) a tooth or teeth can be placed on the implant. The amount of time required to place an implant will vary depending on the experience of the surgeon, quality and quantity of the bone and the difficulty of the individual situation (usually between 30 minutes and 2 hours).
Preparation of recipient bone for implant insertion
Surgical procedure
An incision is made over the crest (highest point of the gum ridge) of the site where the implant is to be placed. The gum (which is referred to as a ‘flap’) was raised to exposed the recipient bone. Then, a pilot hole is bored into the bone, taking care to avoid the vital structures. Drilling into jawbone usually occurs in several separate steps. The pilot hole is expanded by using progressively wider drills (typically between three and seven successive drilling steps, depending on implant width and length). Care is taken not to damage the bone cells by overheating. A cooling saline or water spray keeps the temperature of the bone to below 47 degrees Celsius.
[hana-flv-player
video=”https://prestige-dental-care.com.my/wp-content/uploads/2010/12/Implant-surgical-procedure.flv”
width=”350″
height=”270″
description=”Implant placement procedure”
clickurl=”https://prestige-dental-care.com.my”
clicktarget=”_blank”
player=”4″
autoplay=”false”
loop=”true”
autorewind=”true”
/]
Implant insertion into recipient bone
The implant screw can be self-tapping, and is screwed into place at a precise torque so as not to overload the surrounding bone (overloaded bone can die, a condition called osteonecrosis, which may lead to failure of the implant to fully integrate or bond with the jawbone). Typically in most implant systems, the osteotomy or drilled hole is about 1mm deeper than the implant being placed, due to the shape of the drill tip. Surgeons must take the added length into consideration when drilling in the vicinity of vital structures.
Before implant insertion
After implant insertion on the upper right area
For Anxiety Patient…
If in a case of an anxious patient come for implant placement, usually, we will prescribe some medication of reduce anxiety before the surgery or patient will have to inhale nitrous oxide during the procedure so that he/she will feel relax and calm all the time during surgery. If the patient is extremely phobia of surgery, then he can opt for surgery done under general anaesthesia which required hospitalization.
Healing time
Practitioners usually allow 2–6 months for healing. If the implant is loaded too soon, it is possible that the implant may move which results in failure. The subsequent time to heal, possibly graft and eventually place a new implant may take up to eighteen months. For this reason many are reluctant to push the envelope for healing.
Wound healing – immediate after surgery
Wound healing – 7 days after surgery
One-stage or two-stage surgery?
When an implant is placed with a ‘healing abutment’, which comes through the mucosa (or the gum), it is referred as the one-stage surgery. (Picture above is one-stage surgery where the healing abutment – green and purple screw can be seen on the gum surface)
When an implant is placed with a ‘cover screw’ which is flush with the surface of the dental implant and usually hidden under with the gum, this surgery is referred as the two-stage surgery. A second surgery is needed 3 months later to exposed the cover screw and the cover-screw is to be placed with healing abutment. Two-stage surgery is sometimes chosen when a concurrent bone graft is placed or surgery on the mucosa may be required for esthetic reasons. Some implants are one piece so that no healing abutment is required.
In carefully selected cases patients can be implanted and restored in a single surgery, in a procedure labeled as “Immediate Placement“. In such cases a provisional prosthetic tooth or crown is shaped to avoid the force of the bite transferring to the implant while it integrates with the bone.
Surgical timing
There are different approaches to place dental implants after tooth extraction. The approaches are:
Immediate post-extraction implant placement.
Delayed immediate post-extraction implant placement (2 weeks to 3 months after extraction).
Late implantation (3 months or more after tooth extraction).
Restoration Procedure
For missing single tooth
Implants can be made to replace missing tooth or teeth. If an implant is used to replace one missing tooth, it is implant-supported crown.
Implant-supported crown is used to replaced a missing tooth
Multiple missing tooth
Implant-supported crown can be used to replaced multiple missing tooth. Every missing teeth will be replace with implants
Implant-supported crown
If in cases where the bone is too narrow and not suitable for implant placement then implant-supported bridge will be used to avoid those unsuitable area.
Implant supported bridge
Implant-supported bridge also can be used to reduce implant cost and surgical time!!
Impression taking
After the implant in well osteo-integrated with the surrounding bone, construction of the outer part — the crown/tooth procedure can be started. Usually it started with impression taking after the gum heals around the healing abutment.
Gum healing after a week with healing abutment in two-stage surgery
Impression is used to make a duplication of the gum and the implant position where the laboratory technician can fabricate crown/bridge outside patient’s mouth.
The impression transfer posts are inserted on the implant fixtures
And impression of the gum and implant are taken with silicone material
Crown/Bridge fabrication
In the dental laboratory, porcelain fused to metal crowns or bridges are fabricated. Usually it takes about 2-3weeks to be done.
A model with implant is made from the silicone impression.
On the model, crowns are fabricated and ready to be fit in patient mouth!!
Another case with two implant-supported bridges
Restoration of crown/bridge in the mouth
There are basically 2 types of ways by which the crowns/bridges that can be attached to the implant: Screwed retained – The crowns/bridges are retained in the mouth with screw that screw into the abutment. The advantage of using this way is easy to be removed when ever need (eg. if the crown break or the abutment become loosen). However, the aesthetic will be compromised. Usually screwed retained method is used in posterior region where aesthetic is not an issue or in straight abutment type. Cemented retained – The crowns/bridges are cemented onto the abutment with cement such as temp-bond, GIC etc. The advantages is very good aesthetic. Usually used in the anterior region or in angle abutment type.
Below are the procedures of installing the final restoration of a screw-retained type:
After removing the healing abutment, the implant ‘hole’ will be assessed
The abutments are screwed into the implants with force 15Ncm
Then, the crowns are fit onto the abutments and the colour, shape and occlusion will be assessed
After that, crowns will be screw onto the abutments with force of 15Ncm
The hole at the palatal surface will be covered with filling material
Book an appointment with our doctors now!! Click here
If you have any question, don’t hesitate to contact us, we are more than glad to provide you with the information you need!










![Pre-op01 [1600x1200]](https://prestige-dental-care.com.my/wp-content/uploads/2013/04/Pre-op01-1600x1200.jpg)
![Pre-op03 [1600x1200]](https://prestige-dental-care.com.my/wp-content/uploads/2013/04/Pre-op03-1600x1200.jpg)
![Pre-op02 [1600x1200]](https://prestige-dental-care.com.my/wp-content/uploads/2013/04/Pre-op02-1600x1200.jpg)
![OPG-Pre-ortho [1600x1200]](https://prestige-dental-care.com.my/wp-content/uploads/2013/04/OPG-Pre-ortho-1600x1200.jpg)
![Lat-Pre-ortho [1600x1200]](https://prestige-dental-care.com.my/wp-content/uploads/2013/04/Lat-Pre-ortho-1600x1200.jpg)










































 :
:  :
: 