Gum surgery sometimes needed to correct the gum defect caused by gum disease (such as periodontitist) or gum recession usually due extensive brushing. Gum surgery will helps to impove the gum aesthetically but most importantly, it enable the patient to clean his teeth better.
Different Types of Gum Surgery
There are certain types of gum surgery that usually the dentist will perform depend on the condition of the patient’s gum:
Pocket reduction (Gingiva Flap Surgery) This procedure is indicated for patient with deep pocketing on his gum as the result of gum disease (periodontitist). In this procedure, dentist or periodontist (gum specialist) will reflect the gum to expose the root of deep cleaning and then reposition the gum slightly lower in order to reduce pocket. Thus, this allows the patient to clean his teeth more efficiently.
Regeneration (Guided bone regeneration GBR) When there is excessive bone lost to a single or few teeth in the mouth, the dentist/periodontist might try to ‘re-grow’ the bone back around the tooth. The procedure can be done only after the gum disease ceased. Dentist/periodontist folds back the gums and removes disease-causing bacteria, then inserts bone grafts, membranes, or tissue-stimulating proteins (or any combination of the three) to encourage your gum tissues to regenerate and fit snugly around the teeth again.
Crown lengthening This procedure is done to lengthen the crown of the tooth for restoration later (Example: porcelain crowns or fillings). In cases where the tooth breaks down badly, sometimes, up to the gum level; crown lengthening is performed before restoration. The gum around the tooth will be removed to expose the root. This can be done with laser or electrocautery under local anesthetic. Once the gum healed, the tooth finally will be restore with filling or porcelain crown.
Removing excessive gum (Gingivectomy) In certain conditions where overgrowth of gum covering the teeth (gingiva hyperplasia), gingivectomy can be performed to reduce it. Gingiva hyperplasia usually cause be irritation to the gum, or certain medication patient taking causing the gum grows excessively or can be unknown reason. Basically, gingivectomy improves the teeth aesthetically and reduce plaque accumulation around them.
Soft tissue graft (Gingivoplasty)This procedure is performed on the gum that is thin and receded due to over-brushing. Dentist will take a tissue from elsewhere in your mouth (usually on the palate) and attaches it to your gums to replace gum tissue that has receded or has been removed due to gum disease. This procedure is often used for cosmetic purposes as well as to treat gum disease because it covers areas where the root is becoming exposed and improves the appearance of the teeth.
Is Gum Surgery Painful?
Most people will have only mild to moderate pain after surgery that can be managed with pain relievers. If the is moderate swelling on the gum, cold pack can be used to reduce it. Usually the dentist will give instructions on managing the wound after surgery.
Unfortunately, not all extractions can be done by simply grasping the tooth with forceps and rocking it out. What if there is nothing left above the gum line to grasp? Or what if the crown breaks off leaving the roots still in the bone? These things can and do happen, and any dentist that extracts teeth will have to deal with them routinely.
Retain Root
In these cases, it becomes necessary to surgically remove the tooth. This is frequently accomplished by prying the root out using a sharp instrument that can be forced between the root and the bone surrounding it. This technique is called “luxation“. In the case of multiple rooted teeth, the roots are first separated so they can be removed individually. Unfortunately, not all roots or root fragments may be removed in this fashion. This means that the dentist must make an incision into the gums around the tooth and raise a flap of tissue exposing the tooth and its surrounding bone.
Surgical Extraction – a. Gum flap is raised and surrounding bone is removed. b. The roots of the molar are split with a drill and removed. c. The flap is held back in place with sutures
Sometimes, after the flap is raised, there is enough tooth exposed to grab and remove it as in a simple extraction. Sometimes, the technique described above as luxation may successfully remove the tooth. If luxation fails, the dentist must take a handpiece (drill) and cut away some of the surrounding bone in order to gain a purchase on the tooth. After the tooth has been pried out of the artificially enlarged socket, the dentist then sutures (sews) the flap of tissue back in place so that healing can proceed normally.
Lateral cephalometric is a radiograph of the head taken with the x-ray beam perpendicular to the patient’s sagittal plane. This radiography image is useful for studying the dental and facial growth of a patient.
Position of patient from the X-ray source to produce a standard Lateral cephalometric radiograph
In orthodontic treatment, clinician/orthodontist use this radiograph to identified dental and skeletal deformity; the relationship between upper and lower teeth and jaw bone. By doing so, he can create a treatment plan to correct the teeth misalignment. This radiograph is also useful in monitoring the progress of braces treatment and to compare before and after treatment.
Patient’ head is in ‘natural head position’
During radiograph taking, the patient’s head is positioned in the most relax position — natural head position — is a standardized orientation of the head that is reproducible for each individual and is used as a means of standardization during analysis of dentofacial morphology both for photos and radiographs.
An example of a standard Lateral Cephalometric Radiograph
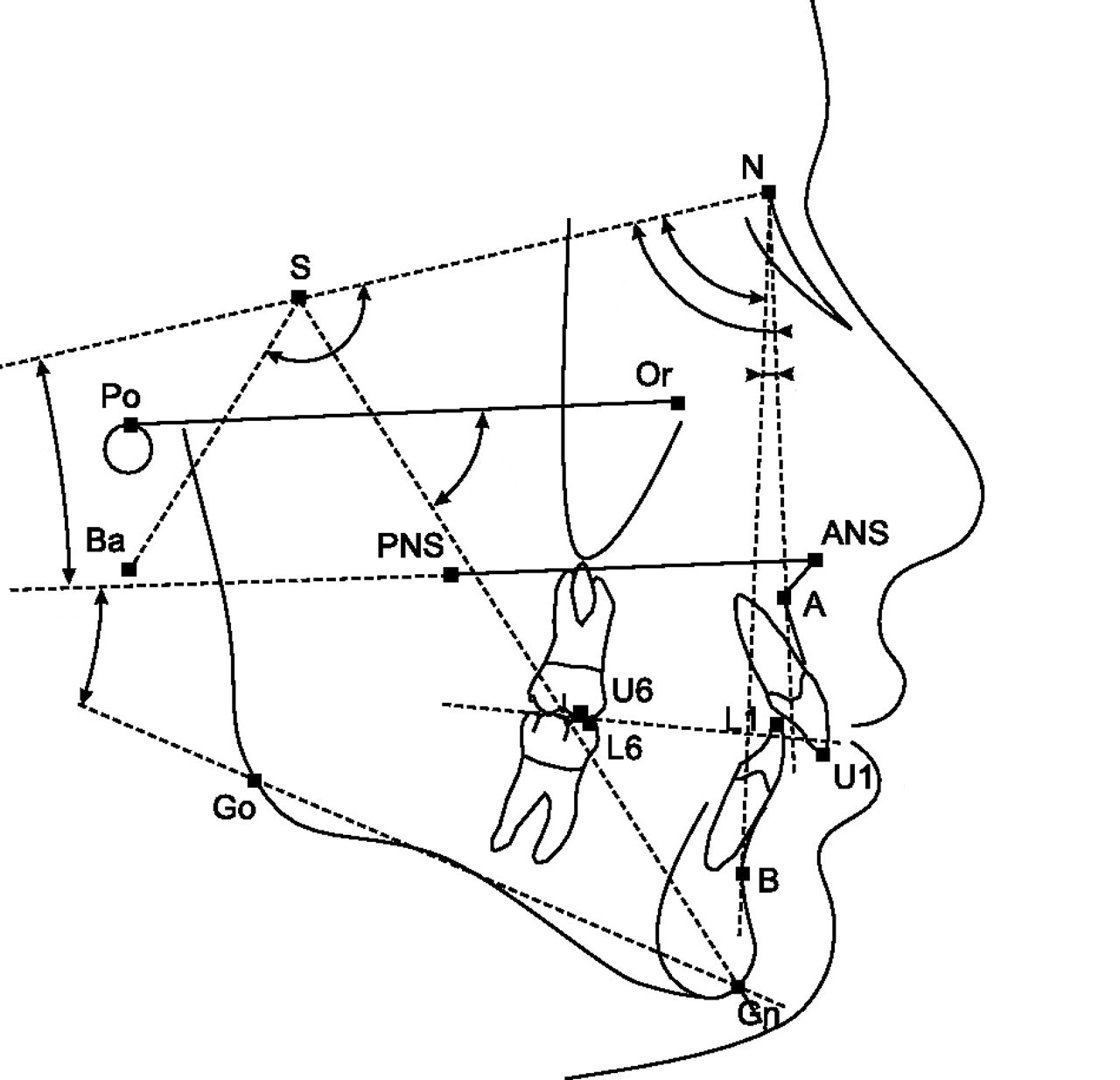
Cephalometric Tracing
Cephalometric tracing is an overlay drawing produced from a cephalometric radiograph by digital means and a computer program or by copying specific outlines from it with a lead pencil onto acetate paper, using an illuminated view-box. Tracings are used to facilitate cephalometric analysis, as well as in superimpositions, to evaluate treatment and growth changes.
The landmarks on the radiograph are identified and marked.
Lines are made to join the markings and the angles where the lines intercept will be recorded. The values of the angle will be compared to the norm value according to the patient’s race. And finally, a conclusion will be depends on the deviation of the patient’s value to the norm value.
Sometimes, lateral cephalometric radiograph can be use to compare before and after treatment or the growth pattern of a child. For example, in the image below, the green line represent before treatment and the black will be after treatment. From here, we can appreciate how the teeth and jaws move during treatment. Doctor use this radiograph to evaluate if he has achieve his treatment objective!!
Dental Panoramic Tomogram or OPG is a sophisticated x-ray machine used to take radiographic images of the teeth and jaws bone which is in a arch position. We used to call this machine as OPG (which stands for ORTHOPANTOGRAM), which was named after the first x-ray unit. OPG performed by using a technique called “tomography”.
The X-ray tube moves around the head, the x-ray film moves in the opposite direction behind your head. This generates an image slice where the mandible and teeth are in focus, and the other structures are blurred.
Our OPG unit in Bandar PuteriPatient is in the standing position when taking OPG
Anatomy The anatomy consists of the body, ramus and angle of mandible, coronoid process, mandibular notch, condyle of mandible, alveolar ridge, symphysis menti, maxillary sinuses, nasal fossae and 16 upper and 16 lower teeth, as shown in the image below.
An OPG image with the anatomical landmark
Reasons for OPG requests
Dental Disease
Caries – appear as different shaped areas of radiolucency in the crowns or necks of teeth.
Peridontioiditis – when inflammation extends into the underlying alveolar bone and there is a loss of attachment.
Peridontal Abscess – Radiolucent area surrounding the roots of the teeth.
Impacted or embedded teeth (eg. wisdom teeth)
OPG shows angulation, shape of roots, size and shape of crown, effect on other teeth.
To look for impacted canine
Teeth Abnormalities
Eg. Developmental, to show size, number, shape and position.
Lesions in the jaw bone
Cyst of jaw bone – shape, size, extension, involving nearby structure
Tumour/growth – benign, malignant
Trauma to teeth and facial skeleton
Mandible fractures are often bilateral.
Panoramic view of mandible to view the fracture.
Determine site and direction of fracture lines.
Relationship of teeth to fracture lines.
Alignment of bone fragments after healing.
Evidence of infection or other complications post intervention.
Follow up to assess healing.
Planing for implant placement
To identify the position and location for implant placement
Bone quality and quantity
Anatomical structure that should be avoided such as the maxillary sinus and the inferior dental nerve
Dental intra-oral radiographs a.k.a X-rays. Dentists use radiographs for multiple reasons: to find hidden dental structures, malignant or benign masses, bone loss, and cavities.
How does x-ray of your teeth formed?
X-ray of your teeth is formed by a controlled burst of X-ray radiation which penetrates oral structures at different levels, depending on varying anatomical densities, before striking the film or sensor.
Teeth appear lighter because less radiation penetrates them to reach the film.
Dental caries, infections and other changes in the bone density, and the periodontal ligament, appear darker because X-rays readily penetrate these less dense structures.
Dental restorations (fillings, crowns) may appear lighter or darker, depending on the density of the material.
Should Patients Have Concerns About Radiation Exposure?
The dosage of X-ray radiation for dental is typically safe, around 0.150 mSv for a full mouth series, according to the American Dental Association website. It is equivalent to a few days’ worth of background environmental radiation exposure, or similar to the dose received during a cross-country airplane flight (concentrated into one short burst aimed at a small area).
Incidental exposure is further reduced by the use of a lead shield, lead apron, sometimes with a lead thyroid collar. Operator exposure is reduced by stepping out of the room, or behind adequate shielding material, when the X-ray source is activated.
Types of intra-oral radiographs
Bitewing
Periapical
Bitewing radiograph
Bitewings
Bitewing radiograph designed the placement of the film packet to reveal the coronal halves of the maxillary and mandibular teeth, inter-proximal contacts and portions of the interdental septa.
It is indicated primarily to detect or monitor interproximal caries if the proximal surfaces of the teeth cannot be visually or tactilely examined.
Occlusal caries, crestal alveolar bone level and secondarily for eruption patterns, caries and restoration proximity to pulp spaces, primary molar furcation pathology and developmental anomalies may also be detected with bitewing radiographs.
Periapical Radiograph
PA radiography describes intra-oral techniques designed to show individual teeth and the tissues around the apices. Each image usually shows two to four teeth and provides detailed information about the teeth and the surrounding alveolar bone.
Anterior PA
Posterior PA
Indications for PA radiograph are:
Detection of apical infection/inflammation
Assessment of the periodontal status
After trauma to the teeth and associated alveolar bone
Assessment of the presence and position of unerupted teeth
Assessment of root morphology before extractions
During endodontics
Preoperative assessment and postoperative appraisal of apical surgery
Detailed evaluation of apical cysts and other lesions within the alveolar bone
Types of dentureBasically, denture (false teeth) is prosthesis device to replace missing teeth. The denture is supported by the surround soft and hard tissue. It is the most economical and easy-to-make prosthesis. Denture can be further divided into complete denture (denture to replace all missing teeth) or partial denture (denture to replace a few missing teeth)
Beside denture, there are other options to replace missing teeth:
Root canal treatment or sometimes refers as RCT is a treatment used to repair and save a tooth that is badly decayed or becomes infected. During a root canal procedure, the nerve and pulp are removed and the inside of the tooth is cleaned and sealed. Without treatment, the tissue surrounding the tooth will become infected and abscesses may form (below).
Gum abscess
What is root canal?
Root canal is the term used to describe the natural cavity within the center of the tooth. The pulp or pulp chamber is the soft area within the root canal. The tooth’s nerve lies within the root canal.
A tooth’s nerve is not vitally important to a tooth’s health and function after the tooth has emerged through the gums. Its only function is sensory — to provide the sensation of hot or cold. The presence or absence of a nerve will not affect the day-to-day functioning of the tooth.
What Damages a Tooth’s Nerve and Pulp in the First Place?
Big decay
A tooth’s nerve and pulp can become irritated, inflamed, and infected due to:
deep decay
repeated dental procedures on a tooth and/or large fillings
a crack or chip in the tooth
or trauma to the face.
How does dentist know whether the tooth needs RCT?
There are several symptoms that usually lead dentist to conclude that the tooth requires RCT:
Pain
Tooth Discolouration
Pain which is severe and prolong that affect daily activities
Throbbing pain that usually disturb sleep at night
Feel painful when biting on the affected side
Prolonged sensitivity/pain to heat or cold temperatures (after the hot or cold has been removed)
Discoloration (a darkening) of the tooth
Swelling and tenderness in the nearby gums
A persistent or recurring pimple on the gums (gum abscess)
From dental examination:
Pulp testing
A very large cavity or deep restoration on that tooth
Feels very painful on percussion on that tooth
Not responsive to the vitality test using a Pulp Tester
A radiolucency lesion over the tip of the root on radiograpghic examination
How does Root Canal Treatment done?
Step-by-step of root canal treatment
A) Placing the rubber dam.
After local anaesthetic is given, dentist usually need to “isolate” your tooth. He will first punch a small hole in a sheet of rubber. Then, he will then slip this sheet over the affected tooth and position a small tooth clamp to hold it there. The purpose of a rubber dam is to keep the tooth saliva-free therefore, avoid contamination of bacteria from saliva .
B) Creating the access cavity.
The tooth was isolated using rubber dam and a hole was made (cavity access) to reach the pulp chamber
As a starting point for performing root canal treatment, dentist must first gain access to the nerve space (or the pulp chamber) within the tooth.
He do this by using a dental drill to create an access cavity. This hole will extend into the interior of the tooth to its pulp chamber. It’s the hole through which the dentist will perform their work.
On the molar teeth, the access cavity is made on the chewing surface of the tooth and for the front teeth, the access hole is made on the tooth’s backside.
The overall size of the access cavity will vary according to factors such as the location of the individual canals and how hard it was for the dentist to find them. Additionally, beyond just that portion of the tooth that must be removed for access, the dentist will also need to remove any decay that’s present and any loose or exceptionally fragile tooth parts or fillings.
C) Cleaning and shaping the tooth’s root canals.
The next step of the root canal process involves “cleaning and shaping” the interior of your tooth (the pulp chamber and all root canals). In regard to the cleaning process, its purpose is to remove bacteria, toxins, nerve tissue, and related debris that are harbored inside the tooth.
The shaping process refers to how the tooth’s canals are enlarged and flared, so the have a shape that facilitates the filling and sealing process.
What instruments are used?
Endodontic file
For the most part, a tooth is cleaned and shaped using endodontic files. These files look like straight pins but on closer inspection you will find that their surface is rough, not smooth. These instruments literally are files and are used as such.
How are the files used?
Dentist works the file up and down, with a twisting motion, in each of your tooth’s root canals. This action will scrub, scrape and shave the sides of the canals, thus cleaning and sculpting them. He will perform this same type of action using a series of files, each having a slightly larger diameter.
The idea is that each consecutive file is used to slightly increase the overall dimensions of the root canal. Since some canal contaminates are embedded within a canal’s walls, this enlargement assists with both the procedure’s cleaning and shaping goals.
While performing this work, the dentist will also periodically flush out (irrigate) the tooth. This helps to wash away accumulated debris and contaminants. While a number of different solutions can be used for this purpose, sodium hypochlorite (bleaching agent) is the most common one. An added benefit of bleach is that it is a disinfectant.
Some dentist may have a handpiece that can manipulate the files for them.
Traditionally, files have been hand instruments. This simply refers to the fact that the dentist creates their filing action by manipulating them with their fingers. Some dentist may, however, have a special dental drill (handpiece) that produces the needed file motion for them.
Rotary Endodontic System
As a variation on this same theme, there is yet another type of dental handpiece that produces a cleaning motion by way of holding a root canal file and vibrating it vigorously.
Measuring the length of the root canals.
Determine the length of root canal with a radiograph
The goal of root canal treatment is to achieve cleaning of the entire length of each of the tooth’s root canals, but not beyond.
As a means of determining the precise length of a canal, dentist will use apex locator to get the measurement for the length of the tooth (from the crown to the tip of the root). By doing so, the dentist wouldn’t go beyond during cleaning.
Usually, he will confirm the measurement by taking a x-ray of the tooth with a file placed in the tooth. The x-ray picture will show if the file extends the full length of the canal or not.
D) Sealing the tooth – Placing the filling material.
Once the interior of the tooth has been thoroughly cleansed and properly shaped, it is ready to be sealed (have its hollow interior filled in). In some cases, the dentist will want to place the filling material immediately after they have finished cleaning the tooth. With other cases, they may feel that it is best to wait about a week before performing this procedure.
What type of root canal filling material is used?
Sealing of the root canals
The most frequently used root canal filling material is a rubber compound called gutta percha. It comes in preformed cones whose dimensions match the size (diameter, taper) of the files that have been used to shape the tooth’s canals.
A root canal sealer (a paste) is usually used with the gutta percha. It is either applied to a cone’s surface before it is placed into a canal, or else applied inside the root canal itself before the cone is inserted. Several individual cones of gutta percha may be needed to fully fill the interior of the tooth.
Dentist will warm the gutta percha (either before or after it has been placed into the tooth) to soften it. This way it can be molded to closely adapt to the shape of the tooth’s interior.
As an alternative, a dentist may place the gutta percha via the use of a “gun.” This apparatus is somewhat similar to a hot-glue gun. It warms a tube of gutta percha. The softened material can then be squeezed out into the tooth.
Once your dentist has finished sealing your tooth, they will place a temporary filling, so to seal off the access cavity created at the beginning of your treatment.
How long does root canal treatment take?
The total amount of time that’s needed for a tooth’s root canal therapy will of course hinge on how many appointments are needed (one visit, or two or more) and how long each one will take. Usually, root canal treatment for molar usually take about 3 to 4 visits. Each visit takes around an hour. For the front teeth, usually take fewer visits as they are simpler and located at the front region.
Summary of Root Canal Treatment:
Cases of root canal treatments
RCT on upper left first molar
RCT on lower right first molar
RCT on lower right first molar
RCT on lower rigth first molar
E) Post Root Canal Treatment
At this point, while the individual steps of performing the root canal process have been finished, the tooth’s treatment is not yet complete. The tooth is no longer alive since the pulp has been removed. And this can make the tooth brittle and more prone to fracture.
Therefore, a permanent restoration must still be placed. Choosing the right type of dental restoration, and having it placed promptly, will help to insure the long-term success of the tooth’s endodontic therapy.
There are a few options:
1) Crown (recommended) as it is strong, durable and more aesthetic
2) Dental filling – cheap, can be done on the spot (doesn’t required 2 visits)
F) Final words…
Tooth infection can recur in treated teeth (even RCT treated tooth), hence, good oral hygiene, including brushing, flossing and regular dental examination are necessary to prevent further problems. For more info on good oral hygiene click here.
Root planing is a non-surgical treatment that usually done together with deep dental scaling. It is done after the supragingival (or superficial) plaque and calculus were remove through gross scaling. The aim of this treatment is to removes the roughened cementum and surface dentin that is impregnated with calculus, microorganisms and their toxins leading to the creation of a clean smooth root surface. Usually this implies that some cementum and dentin are removed. Deep scaling and root planing are done under local anaesthesia and requires 25-45 minutes per quadrant. If the pockets are deeper, the procedure becomes more significantly more difficult and more time is needed.
Cosmetic gum surgery – It is a type of surgery used to reshape healthy gum tissue around the teeth to make them look better. If a person has tooth recession where the gum is pushed away from the tooth, a gingivoplasty surgery can be done. Basically to ‘bring’ back the gum to cover the expose root surface of a tooth:
Before cosmetic gum surgery (gingivoplasty surgery) – receding gum especially on patient’s left sideAfter cosmetic gum surgery (gingivoplasty surgery)
To read more on the gingivoplasty procedure click here.
On the other hand, if there is excessive gum covering the teeth, then the procedure is to remove some part of the gum covering the teeth (gingivectomy surgery) to show more of the tooth thus reduce gummy smile and improve smile line.
Before gingivectomyAfter gingivectomy
To read more on the gingivectomy procedure click here.
After gum surgery, it is important that the periodontist or dental hygienist inform you how to clean the teeth and gum tissue with a toothbrush and an antimicrobial fluoride toothpaste, floss and antibacterial mouth rinse. Please consult your periodontal specialist or dentist for more information of how to care for your gum tissue and teeth after gum surgery.
Book an appointment with our doctors now!! Click here
If you have any question, don’t hesitate to contact us, we are more than glad to provide you with the information you need!











































 :
:  :
: 